In addition to evaluations of other charities, GiveWell publishes substantial evaluation on itself, from the quality of its research to its impact on donations. We publish quarterly updates regarding two key metrics: (a) donations to top charities and (b) web traffic.
The charts below present basic information about our growth in money moved and web traffic thus far in 2012. Website traffic tends to peak in December of each year (circled in the chart below). Growth in web traffic has generally remained strong in 2012.
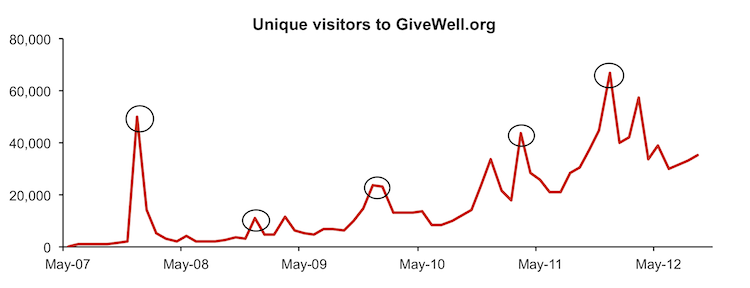
So far in 2012, there have been 342,551 monthly unique visitors (calculated as the sum of unique visitors in each month) to the website, compared with 238,172 at this time in 2011, or 44% annual growth. A significant contributor to this growth was an increase in our Google Grants budget (which provides us free advertising via Google AdWords). Excluding this, we have had 23% annual growth in web traffic.
Growth in money moved has remained strong as well. The majority of the funds GiveWell moves come from a relatively small number donors giving larger gifts. These larger donors tend to give in December, and we have found that growth in donations from smaller donors throughout the year tends to provide a reasonable estimate of the growth from the larger donors by the end of the year.
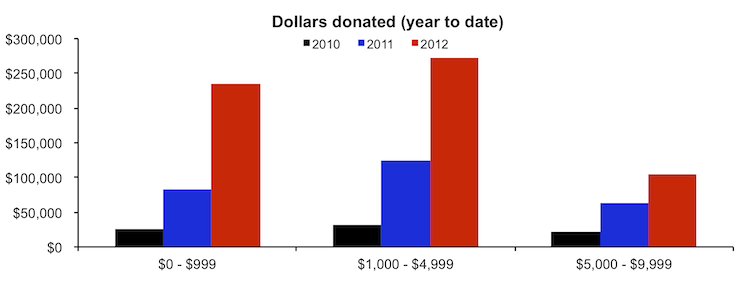
Below, we show two charts illustrating growth among smaller donors.
Thus far in 2012, GiveWell has directed $604,327 to our top charities from donors giving less than $10,000. This is approximately 2.4x the amount we had directed at this point last year.
Most donors give less than $1,000; the chart below shows the growth in the number of smaller donors giving to our top charities.
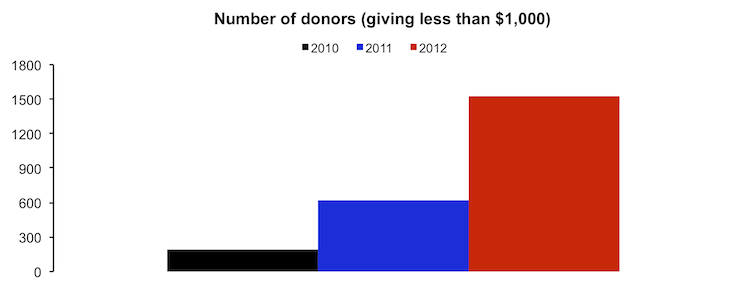
Overall, 1531 donors have given to GiveWell’s top charities this year (compared to 624 donors at this point last year).
In total, GiveWell donors have directed $1,394,071 to our top charities this year, compared with $766,561 at this point in 2011. For the reason described above, we don’t find this number to be particularly meaningful at this time of year.